






Parasitology Basic 08d
- 1. Parasitology - Basic Science Paul A. Gulig, Ph.D. I. Parasitism - A relationship between organisms where one (the parasite) gains food and shelter from another (the host) which suffers from the relationship. This is opposed to mutualism where both benefit or commensalism where one gains but the other is not harmed.
- 2. II. Types of organisms - A. protozoa - single celled eukaryotes 1. intestinal and urogenital 2. blood and tissue B. helminths (worms) 1. cestodes (tapeworms) 2. trematodes (flukes) 3. nematodes (roundworms) C. arthropods 1. Cimex lectularius (bed bug)
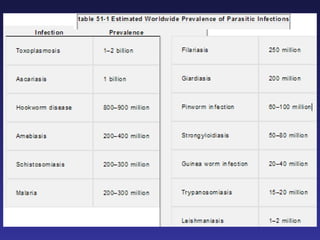
- 3. III. Importance - Table 51-1 A. Billions of cases worldwide - lots of morbidity B. Malaria causes over 1 million deaths/year C. There ARE many parasitic diseases endemic to the U.S. – Table 51-2 D. Even for those that are not endemic - travelers and immigrants bring them here.
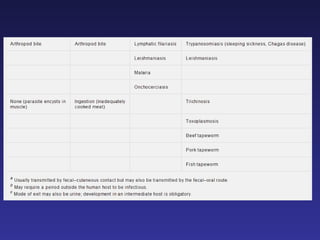
- 5. Pathogenesis A. Encounter 1. Geographic distribution - regions of world as well as regions of U.S. 2. One or more hosts (notice difference between simple vectors versus replication within the non-human host) 3. Arthropod vectors – bites 4. Oral (food and water)
- 6. 5. Direct penetration of intact epidermis (different from bacteria and viruses) 6. Some are human only 7. Occupational, activity relationships 8. Considered exogenous infections (although some are often asymptomatic, depending on conditions, not considered normal flora)
- 7. B. Entry (Table 51-3) 1. Oral, epidermis, bites, sexual 2. Specific adherence by protozoans just like bacteria 3. Worms - biting, sucking mouthparts
- 10. C. Spread 1. Some do, some don't 2. Some travel through body in a complex, orderly process 3. Tissue specificity often seen
- 11. D. Evade defenses 1. Most of these are chronic infections; therefore evasion of even specific adaptive immunity is important 2. Antigenic mimicry, Antigenic cloaking (masking), Antigenic variation 3. Nonspecific generalized stimulation of immunoglobulin
- 12. E. Multiplication 1. Often specific to different hosts, dependent on life cycle form 2. Inappropriate host causes special forms of disease 3. Not often cultured
- 13. F. Damage 1. Generally no toxins, except damaging enzymes 2. Parasite burden in tissue (migration, blockage, pressure) 3. Immunologic a. Inflammation b. Type 1: Hypersensitivity reactions c. Type 2: Cytotoxicity d. Type 3: Immune complex e. Type 4: DTH – CMI
- 14. F. Damage 4. Bleeding and loss of blood 5. Cysts, etc. in tissues 6. Allowing spread of bacteria from gut 7. The infective dose often directly relates to severity of disease (e.g., a few worms is no big deal, many worms can be lethal) 8. Repeated encounter can be additive
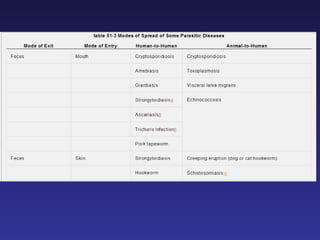
- 15. G. Move to new host (Table 51-3) 1. Direct human to human 2. Human to animal/vector to human 3. Human dead end (accidental) host
- 16. Diagnosis A. Most often seeing organism in patient sample (macroscopic - worms, microscopic - others) 1. Feces, urine, blood, biopsy, endoscopic, Entero (string) test 2. Radiographic observation of damage 3. Eosinophilia - only seen with tissue-invasive worms 4. Serology 5. Nucleic acid-based coming soon
- 17. VI. Treatment A. Because eukaryotic and highly varied life forms - new sets of drugs B. Some antibacterials still useful C. Need to know general classes, few specific examples, mechanisms of action, toxicities
- 18. 1. Anti-protozoals (inhibit replicating organisms, similar to bacteria) a. Heavy metals - arsenic and antimony - Leishmania b. Aminoquinolones (numerous targets) - chloroquine, quinine - Malaria c. Trimethoprim, sulfa drugs - Folic Acid - Toxoplasma, Malaria d. Protein synthesis - Malaria, Babesia, Entamoeba, Cryptosporidium e. Metronidazole - DNA - Entamoeba, Giardia, Trichomonas f. Quinolones - Ciprofloxacin - Malaria
- 19. 2. Anti-helminth (disrupt adults) a. Mebendazole, thiabendazole - microtubule - broad spectrum b. Pyrantel pamoate - muscle relaxant - Ascaris, Enterobius, Hookworm c. Piperazine - muscular paralysis - Ascaris, Enterobius d. Ivermectin - muscular - Filaria e. Niclosamide - oxidative phosphorylation - Cestodes f. Praziquantel - muscle, tegument - Broad spectrum
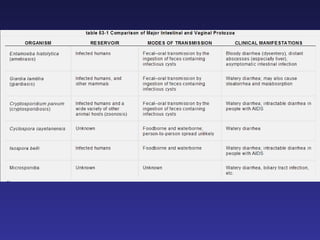
- 20. SPECIFIC AGENTS AND DISEASES I. Protozoa A. Urogenital - Trichomonas vaginalis - already covered by Dr. Poff B. Intestinal protozoa (Table 53-1) 1. Entamoeba histolytica - amoebic dysentery, invasive disease 2. Giardia lamblia – non-invasive diarrhea 3. There are numerous commensal ( normal flora ) intestinal amoeba (don't memorize names) 4. Two cellular forms - trophozoites (replicating) and cysts (survival outside host)
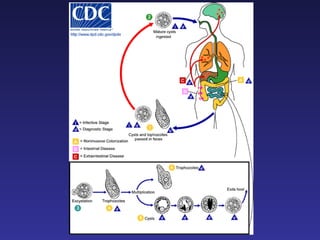
- 22. C. Entamoeba histolytica (life cycle Fig. 53-1) 1. Amoebic dysentery : abdominal pain, cramps, diarrhea, dysentery, bloody stools, colitis 2. Liver and systemic infection - fever, leukocytosis, rigors 3. Encounter a. worldwide - temperate – developing (5-10% carriers); U.S. (1 - 2% carriers) b. fecal-oral (hygiene, sanitation), cysts in stool, trophs in intestine and tissues
- 23. 4. Entry - Ingestion of cysts - trophs in large intestine - specific adhesin 5. Spread – Yes - invasive of gut epithelium - even to liver and elsewhere 6. Evasion of defenses a. Killing of PMNs and macrophages b. IgG/IgA protease
- 24. Trophozoite with ingested RBCs
- 26. 6. Damage a. Cytotoxin b. Flask-shaped ulcers in gut c. Secondary bacterial infection from invasion d. Liver abscess 7. Move to new hosts - yes - cysts in feces 8. Treatment – metronidazole 9. Diagnosis – a. microscopy Cysts in stool, biopsy, ingested RBCs definitive b. serology in U.S.
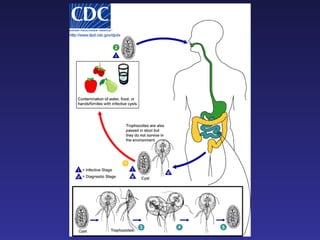
- 27. D. Giardia lamblia - flagellate (life cycle Fig. 53-2) 1. asymptomatic to mild diarrhea to severe diarrhea (cramps, gas, smell, steatorrhea), 10-14 days or longer 2. Encounter a. worldwide including U.S. i. sylvatic from animals ii. human-human fecal-oral , hygiene, sanitation, sexual b. cysts in water
- 28. 3. Entry a. stomach acid – cyst to trophozoite b. attach to small intestine with sucking disk 4. Spread - none
- 29. Trophozoite
- 31. 5. Damage - malabsortion diarrhea 6. Move to new hosts - yes - fecal-oral, sexual 7. Treatment – Metronidazole 8. Diagnosis - Cysts or trophs in stool, string test
- 32. E. Blood and tissue protozoa (Table 52-1) 1. Plasmodium species - we will concentrate on the most common ( P. vivax ) and most lethal ( P. falciparum ) a. malaria - complex life cycles with sexual and asexual cycles in different hosts b. over 1 million deaths/year - mainly Africa (life cycle Fig. 52-1) c. Incubation period - 8-30 days, depending on species d. influenza-like symptoms; paroxysms (fever, chills, rigors) every 36 to 48 hours, depending on species e. sickle cell trait and P. falicparum
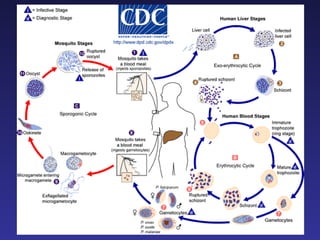
- 33. f. Encounter i. Not endemic to U.S. (imported cases, but few mosquito reported) - tropics, subtropics ii. mosquito bite (Anopheles) with sporozoites (U.S. does have Anopheles); prevent encounter with mosquito g. Entry and Spread - circulatory system to liver
- 34. h. Multiplication - liver (exoerythrocytic) - schizogony (asexual) i. release merozoites into blood that infect RBCs (erythrocytic cycle - more asexual) ii. differentiation into gametocytes - blood meal for mosquitoes ( sexual cycle ) iii. P. vivax only invades young , immature RBCs iv. P. falciparum no specificity for RBCs (more infected cells, more severe disease)
- 37. i. Evasion of defenses i. intracellular shielding ii. antigenic variation of major surface protein (MSP-1)
- 38. j. Damage i. both - lysed hepatocytes , RBCs , plugged capillaries ii. P. falciparum - RBCs adhere to capillaries including brain, RBC lysis, kidney ( blackwater fever ); more deaths
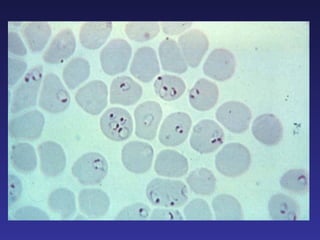
- 39. k. Diagnosis - microscopic examination of blood smears (Fig. 52-3) i. P. falciparum – numerous rings/RBC and high number of infected RBCs, no Schüffner dots ii. P. vivax – single ring/RBC and lower number of infected RBC, has Schüffner dots l. Treatment - chloroquine and primaquine, among others
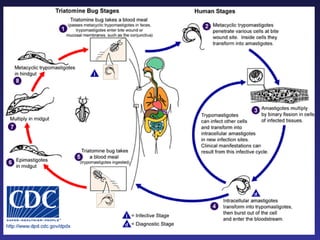
- 40. 2. Trypanosoma cruzi (life cycle Fig. 52-8) - Chaga's Disease a. Disease - i. asymptomatic - mostly ii. acute - rash, edema on face (site of bite), flu-like symptoms – most common when symptoms occur, but acute can cause death iii. chronic – rare but serious ● g.i. tract nerve damage leading to megacolon ● heart - conductive problems and cardiomyopathy, sudden death
- 41. b. Encounter - South, Central, North America, rare in U.S. (southern states) i. "kissing bug" reduviid bug vector (epimastigote replicative form) c. Entry, Spread, Multiplication i. bug defecates on wound releasing trypomastigotes that get rubbed into wound and vasculature ii. convert to amastigotes that invade and replicate in host cells
- 43. d. Damage – unclear mechanism i. fibrosis (autoimmunity?) ii. nerve damage e. Diagnosis – clinical, serology, blood smear microscopy f. Treatment - not very good, especially for late complications g. Prevention – clear houses of bugs, use netting for sleeping
- 44. II. Helminths – worms see Tables 54-1, 54-2, 55-1 for summary
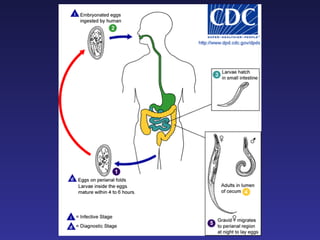
- 45. A. Nematodes (roundworms) (Fig. 54-1) 1. Enterobius vermicularis (small pinworm - 1 mm) (life cycle Fig. 54-3) a. asymptomatic to perianal itching, pruritis b. Encounter - in U.S. - ingestion of egg c. Entry - larvae from small intestine to large intestine d. Spread - none - intraluminal only
- 46. e. Multiplication - adults in large intestine , female migrates to anus to lay eggs at night f. Move to new hosts - yes - stable eggs in environment, scratching, autoinfection prevent by cleanliness g. Diagnosis - scotch tape test – eggs from perianal region in morning h. Treatment - pyrantel pamoate, mebendazole
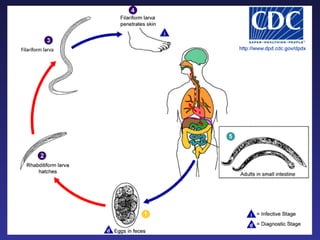
- 49. 2. Hookworms - Ancylostoma duodenale and Necator americanus (Life cycle Fig. 54-4) - 700,000 infected in U.S. a. Symptoms i. allergic reaction in feet upon entry through skin (temporary ground itch) ii. pneumonitis during migration through lungs iii. g.i. - nausea, vomiting, diarrhea iv. anemia due to feeding of adult worms in intestines
- 50. b. Encounter and Entry i. Filariform larvae in soil from human feces ii. Need warm, moist soil - southern U.S. iii. Penetrate intact skin (unusual fecal-cutaneous route) c . Spread and Multiplication i. Circulation ii. Lungs iii. Coughed, swallowed iv. Adults intestines v. Feed off blood vi. Eggs in feces
- 52. d. Damage i. skin penetration ii. lung migration iii. blood loss e. Move to new human host – yes f. Diagnosis - Observe characteristic eggs in stool g. Treatment - mebendazole; pyrantel pamoate h. Prevention - hygiene, sanitation, shoes
- 53. 2. Strongyloides stercoralis (life cycle Fig. 54-4) a. Strongyloidiasis - asymptomatic to pneumonitis (migrating larvae) heavy loads - bowel inflammation and ulceration, diarrhea, vomiting, sepsis
- 54. b. Encounter and Entry - in warm regions of U.S. (but also North) i. mainly human , but some animals possible including pets ii. fecal contamination iii. penetration of intact skin by filariform larvae in soil
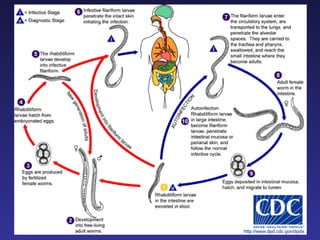
- 55. c. Spread and Multiplication i. filariform larvae invade from skin to blood to lungs to stomach to intestines ii. mature to adults in intestines release eggs hatch to rhabditiform larvae (not invasive) iii. rhabditiform larvae in soil mature to either free-living adults (different from hookworms) or filariform (infective) larvae
- 57. d. Damage i. migrating larvae in lungs; adults in intestines ii. autoinfection - rhabditiform in intestines mature to filariform (rare) - bacterial infection because of gut invasion
- 58. iii. hyperinfection - >80% mortality - drugs, immune suppression - rhabditiform larvae change to filariform in host (large scale) - screen transplant or immune suppressed patients - lung symptoms common, but can go anywhere - bacterial infection because of gut invasion
- 59. e. Move to new human hosts - yes - rhabditiform larvae, eggs in feces f. Diagnosis - observe rhabditiform larvae in stool, eggs rare, eosinophilia g. Treatment - thiabendazole
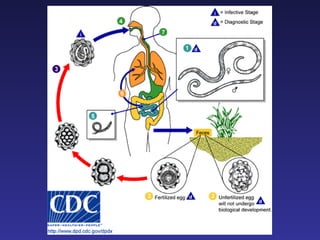
- 60. 3. Ascaris lumbricoides (large roundworms - 20-35 cm) (life cycle Fig. 54-2) a. ascaris infection - over 1 billion worldwide! b. few worms - no symptoms heavy burden - respiratory, blockage c. Encounter - human only, ingestion of egg ; poor sanitation; warm climate
- 61. d. Entry - Oral , filariform larvae in small intestine e. Spread - yes – i. larvae penetrate intestinal wall ii. into blood iii. eventually to lung iv. coughed up v. swallowed
- 63. f. Multiplication - adults - small intestine - eggs g. Damage i. pneumonitis if many worms in lungs; peritonitis (bacteria) ii. occlusion of intestines iii. danger of induced migration by other treatments
- 64. h. Spread to new hosts - yes - fecal oral i. Diagnosis - eosinophilia ; eggs in stool j. Treatment - mebendazole
- 65. 6. Ancylostoma braziliense ( dog/cat hookworm ) Life cycle Fig. 54-4, see Table 55-1) a. Cutaneous Larva Migrans, creeping eruption, ground itch
- 66. b. Encounter, Entry, Spread, Multiplication i. found in warm regions of U.S. ( here ) ii. contamination of soil with animal feces containing filariform larvae iii. larvae penetrate skin and migrate iv. cannot differentiate
- 67. c. Damage - create tracks of migration for weeks to months d. Diagnosis - clinical, eosinophilia e. Treatment – thiabendazole f. Prevention - pet owner education - cover the sandbox
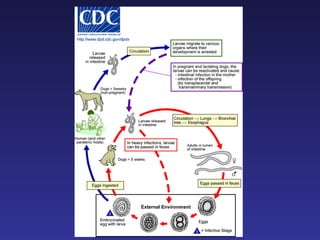
- 69. 7. Toxocara canis and T. cati (See Table 55-1) Dog and cat ascarid worms - inappropriate human infection a. visceral larva migrans b. Encounter - dog and cat definitive hosts, ingestion of eggs from feces c. Entry – oral d. Spread - yes - larva migrate through tissues but do not develop further
- 70. e. Mulitplication - No - wrong host f. Damage - migration of larvae through tissues, inflammatory response g. Diagnosis i. eosinophilia ii. epidemiology (dogs/cats) iii. symptoms (depends on worm burden) iv. serology
- 71. h. Treatment - anti-worm, corticosteroids i. Prevention - keep animal feces out of mouth !
- 72. B. Cestodes (tapeworms) (Life cycle 54-5) 1. General characteristics a. body segments: head = scolex , others proglottids b. no intestines - absorb nutrients c. hermaphroditic (don't need male and female in same host) d. complex life cycles - pay attention to forms encountered by different hosts e. usually asymptomatic, except passage of proglottids in stool , possible nausea
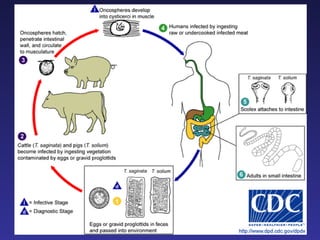
- 73. 2. Taenia solium ( pork ) - rare in U.S. Taenia saginata ( beef ) - common in U.S. Diphylobothrium latum ( fish ) – common a. Encounter - ingest meat with larvae of worm ( cysticercus ) b. Entry - Oral - larvae mature to adult in intestine c. Spread – No
- 74. d. Multiply i. proglotids can mutliply to form chains several meters long ii. break off and are excreted in feces
- 75. e. Damage - consumption of nutrients in intestines ( vitamin B12 for D.l., some intestinal irritation f. Move to new host i. Taenia - eggs ingested by pigs/cows , migrate into tissue and form larvae ii. D.l. more complicated - intermediate in copepod eaten by fish to form larvae
- 77. g. Diagnosis - eggs in stool h. Treatment – niclosamide i. Prevention - sanitation
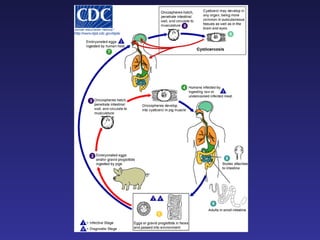
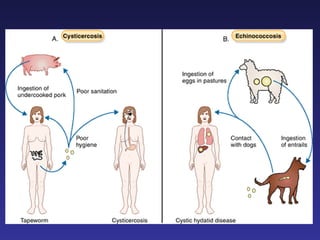
- 78. 1. Cysticerosis – inappropriate infection by pork tapeworm only (life cycle Fig. 54-5, 55-4, see Table 55-1) a. asymptomatic to mental problems, depending on burden and site
- 79. b. Encounter and Entry i. ingestion of egg of Taenia solium (pork tapeworm) in human feces – prevalent in Mexico ii. eggs hatch in stomach releasing onchosphere iii. autoinfection by ingestion of eggs released by tapeworm infection or regurgitation of eggs into stomach from intestines iv. compare with ingestion of larval stage (cysticerci) in pork
- 80. c. Spread - onchosphere penetrates intestines and migrates in blood to tissues d. Multiplication - none in human by this route (compare with tapeworm infection) - humans are dead-end host (unless someone gets eaten by someone or something!)
- 83. e. Damage - onchosphere develops into cysticercus, which cannot develop further - calcification and inflammation in brain, muscle, eye, heart, lung f. Diagnsosis – eosinophilia, radiology g. Treatment - praziquantel, steroids, surgery
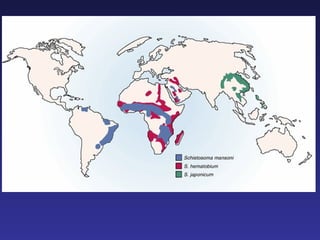
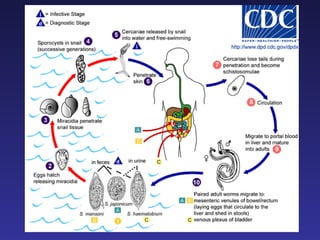
- 84. C. Flukes - Schistosomes - (life cycle 55-7) 1. schistosomiasis : 200 million infections , 3 species 2. Encounter and Entry (Fig. 55-6) a. throughout world, but not in U.S. i. S. mansoni - South America, Africa, Middle East ii. S. japonicum - East Asia iii. S. haematobium - Africa, Middle East
- 86. b. invasion of skin by cercarial forms (some skin symptoms - rash ) 3. Spread a. into blood - portal vein b. mating pairs migrate to terminal tissue i. S. mansoni and S. japonicum - mesenteric veins ii. S. haematobium - urinary bladder
- 88. 4. Multiplication - eggs released a. nonspecific complaints during egg shedding (fever, chills, malaise, inflammation) b. S.m. and S.j. eggs into intestines, liver c. S.h. eggs into bladder 5. Evasion of defenses - antigenic cloaking by binding host proteins
- 89. 6. Damage a. inflammatory and fibrotic response to eggs in tissues b. penetration damage c. S. mansoni and S. haematobium - intestinal and liver symptoms d. S. haematobium - urinary symptoms, bladder cancer correlation
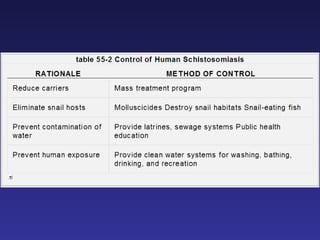
- 90. 7. Spread to new host - indirectly a. shed eggs develop into miracidia that infect snails b. snails release infectious cercaria 8. Diagnosis a. eggs in stool or urine b. eosinophilia 9. Treatment - praziquantel, anti-inflammatories 10. Prevention - sanitation (see Table 55-2)